MLR&O wins Top Doctors 2019
Congratulations Gary V. Gordon, MD, FACP, FACR, Thomas Harder, MD & Amy Lundholm, DO, Main Line Today’s 2019 TOP DOCTOR WINNERS!
MLR&O wins Top Doctors 2019 Read More »
Congratulations Gary V. Gordon, MD, FACP, FACR, Thomas Harder, MD & Amy Lundholm, DO, Main Line Today’s 2019 TOP DOCTOR WINNERS!
MLR&O wins Top Doctors 2019 Read More »
To accommodate our patients, Main Line Rheumatology has increased its hours to better serve you! LANKENAU MEDICAL CENTER Monday 9am – 5:30pm Tuesday and Wednesday 8am- 4pm Thursday 9am – 4pm Friday 8am- 4pm MAIN LINE HEALTH CENTER, Broomall Tuesday, Wednesday and Friday 9am – 4pm
Philadelphia, PA May 9, 2019… Main Line Rheumatology is excited to announce that we have added Hyon Ju Park, MD, to our staff of rheumatologists. Dr. Park has an impressive resume. She is board-certified in rheumatology and internal medicine, and certified in clinical densitometry (bone density studies). Dr. Park graduated Columbia University in 2003 with
Main Line Rheumatology Welcomes New Staff Rheumatologist, Hyon Ju Park, MD Read More »

Main Line Rheumatology sees many patients with osteoporosis. At least 95% are women, yet statistics looking at people over age 65, find the ratio closer to 50%. Why is that? Most women see their gynecologist for a yearly exam, and those doctors are very good about ordering DEXA (bone density) scans. There is no equivalent
Men Get Osteoporosis, Too! Read More »

CONGRATULATIONS! Philadelphia magazine awards Gary V. Gordon, MD, FACP, FACR and Thomas Harder, MD, Main Line Rheumatology, TOP DOCTORS 2019! Main Line Rheumatology has offices at Lankenau Medical Center and Main Line Health Center, in Broomall. In addition to Dr. Gordon and Dr. Harder, our doctors, Amy Lundholm D.O. and Hyon Ju Park, MD, are
Philadelphia TOP DOCTORS 2019 Winners and Still Champions! Read More »
FDA has approved new drug for osteoporosis.
Food and Drug Administration Approves New Osteoporosis Drug That Restores Bone Read More »
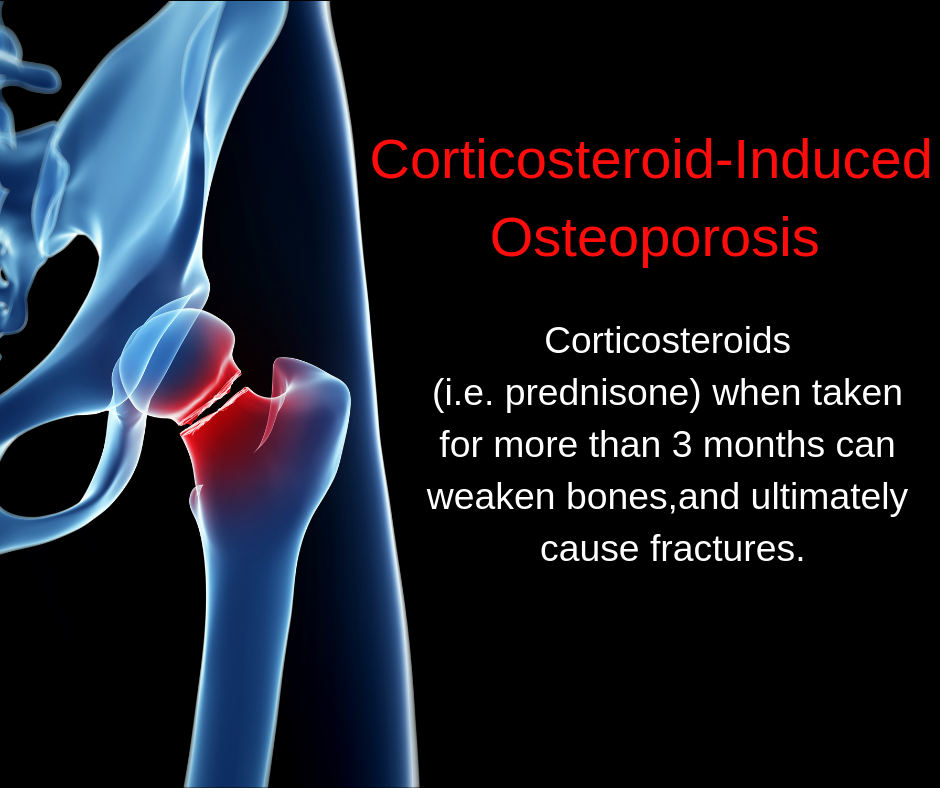
This could be a wake-up call to action! Glucocorticoids or steroid medications taken for many medical conditions to help you feel better, can end up creating a serious bone fracture and disease problem for many adults. The question to ask yourself, and your family doctor or rheumatologist is, “Am I exchanging one problem for another?”
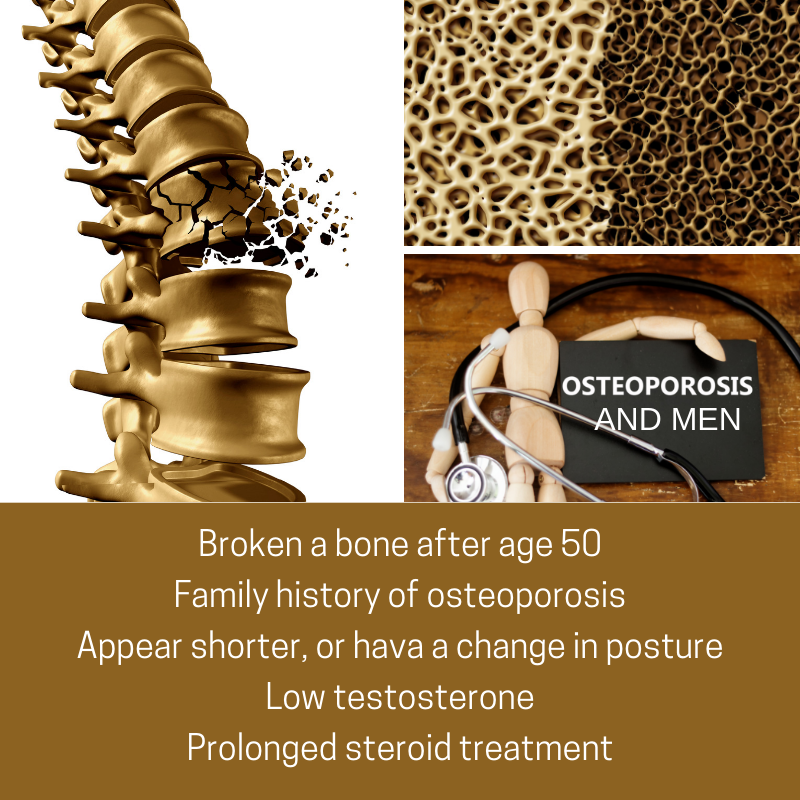
To all men over age 50: At your next annual physical checkup visit, ask your doctor to check your height. If you have lost about one inch or more in the past year, you may have male osteoporosis, and is a very noticeable sign. Osteoporosis is not just a “woman’s disease”. Although osteoporosis is typically
Men and Osteoporosis. It’s Real, and Might Affect You! Read More »

Gary V. Gordon, MD, FACP, FACR, Chief of Rheumatology, Lankenau Medical Center, Wynnewood, PA received the 2018 Rheumatologist of the Year Award from The Arthritis Foundation. He is pictured with Holly Maddams, Executive Director of the Arthritis Foundation, Eastern PA. Dr. Gordon was honored on October 5, 2018 at The Arthritis Foundation’s Bone Bash, held at

Everybody wants to maintain optimal height during their adult lifetime. But height loss is a common part of the aging process. We may notice tall elderly people with great posture, but unfortunately, they are a distinct minority. There are two kinds of height loss. All of sudden at a doctor’s office visit, you find out
Why Am I Height Challenged? Read More »