Gout is a disease that has literally been known to man, since antiquity.
Gout was historically known as “the disease of kings” or “rich man’s disease” especially 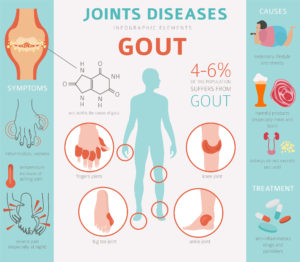 during the Depression, because it was thought to be caused by a “rich” diet, heavy in meat. The first documentation of gout was from Egypt in 2,600 BC, in a description of arthritis of the big toe.
during the Depression, because it was thought to be caused by a “rich” diet, heavy in meat. The first documentation of gout was from Egypt in 2,600 BC, in a description of arthritis of the big toe.
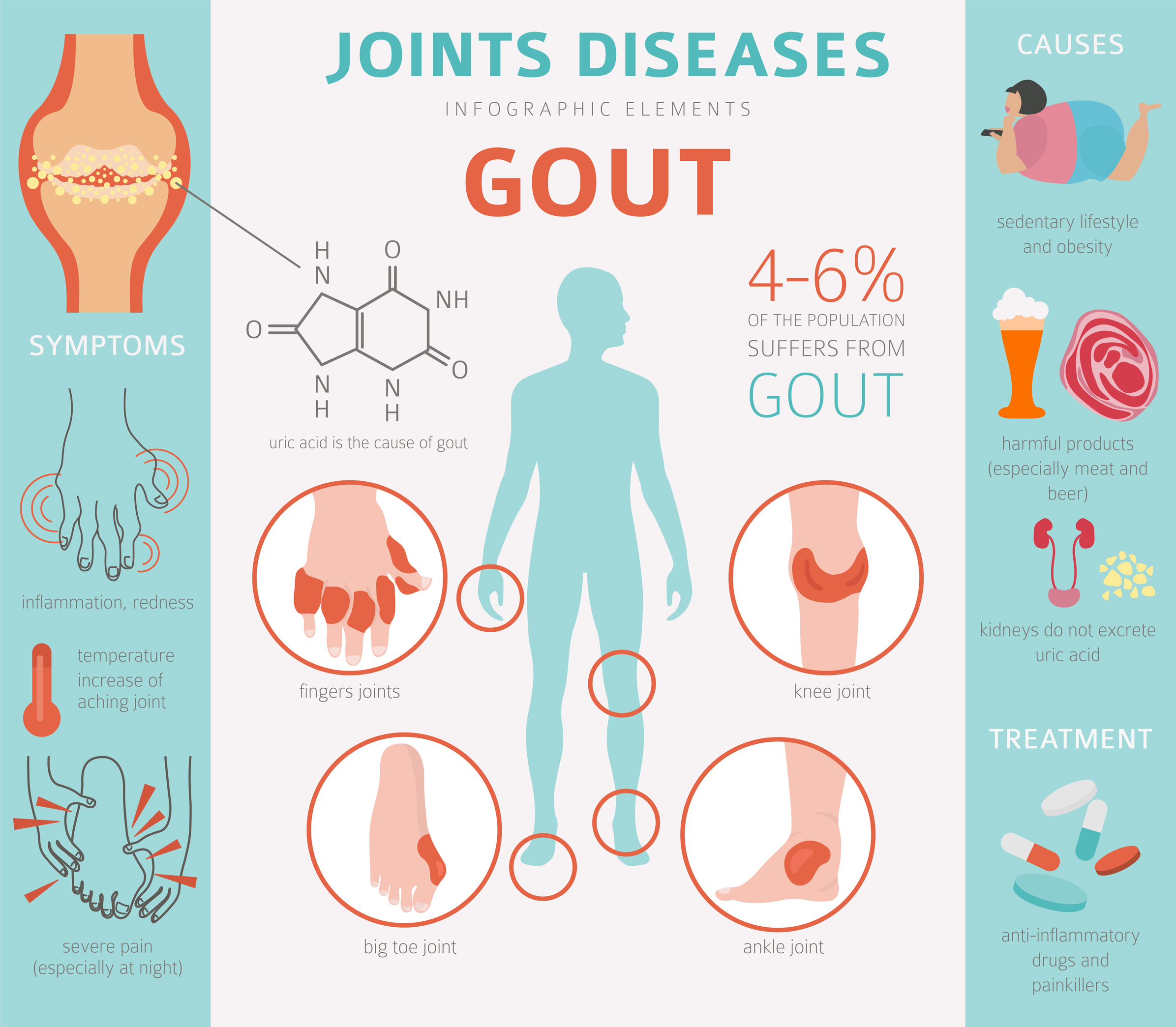
Gout is characterized by recurrent attacks of a red, tender, hot, and swollen joint, often the joint of a big toe. However, any joint can be involved including the spine or rare occasion. The first attack can come on rapidly, out of nowhere and normally intensifies over less than 12 hours. Patients will say that even contact with a bed sheet can be excruciating.
Who gets gout? Gout affects about 1 to 2% of the Western population at some point in their lives, and has become more common in recent decades. Medical risk factors include obesity, diabetes, hypertension, kidney failure and metabolic syndrome, which is a cluster of conditions including high blood pressure, high blood sugar, excess abdominal body fat and abnormal cholesterol or triglyceride levels that together, increase the risk of heart disease, stroke and diabetes. Diuretics, alcohol binge drinking, and certain foods (see below) are risk factors.
Sometimes you just cannot help that you have gout! It is partly genetic as family history increases your risk, and older males are most commonly affected. Gout is no longer considered the “rich man’s disease” as it has no socioeconomic factor.
Approximately 50% of gout cases are due to persistently elevated levels of uric acid the blood. Simply explained, uric acid is a chemical produced when your body breaks down foods that contain organic compounds called purines. Foods and beverages with a high purine content include liver and other organ meats, anchovies, mackerel, dried beans and other legumes, spinach, dried mushrooms, seaweed, high-fructose drinks, beer and wine. Uric acid is eliminated in our urine, but some people cannot eliminate as well as others. When too much uric acid remains in the blood, it can form sharp crystals which deposit in the joints, tissues and tendons, resulting in a “gouty attack”. The more frequently this happens, the more joints tend to be involved with each attack.
A rheumatologist is the best doctor to diagnose and treat gout, since gout is a form of inflammatory arthritis, and rheumatologists are arthritis war czars! It is important to drain fluid from a joint, examine it under a special microscope and establish the diagnosis. This is especially important for short and long term treatment as other medical problems (i.e. joint infections) can look similar. Your rheumatologist will examine, diagnose and treat your gout, while making lifestyle and diet recommendations so you experience fewer attacks.
How does gout present itself, and how do you know when to see a rheumatologist? Gout signs or symptoms present in multiple ways, although the most usual is a recurrent attack of acute inflammatory arthritis with a red, tender, swollen joint that feels hot. The joint at the base of the big toe is affected most often, accounting for 50% of the cases we see, and other joints – heels, knees, wrists, and fingers, may also be affected. Joint pain usually begins over a few hours during the night while sleeping, mainly due to lower body temperature. Sometimes other symptoms may occur along with the joint pain including fatigue, a high fever, or tophi (singular-tophus) which are hard, painless deposits of uric acid crystals in joints, cartilage and bones or other places on the body. Tophi can look very scary to the observer, but are treatable,
Gout treatment is divided into two parts: acute attack medication and prevention. Medication such as non-steroidal anti-inflammatory drugs (NSAIDS) or cortisone will alleviate pain and provide improvement within twenty-four hours. Without treatment, an acute attack of gout usually resolves in five to seven days, however, 60% of people have a second attack within one year. Those with gout are at increased risk of high blood pressure, diabetes, metabolic syndrome, and kidney and cardiovascular disease-thus increased risk of death.
Your gout is treatable and with medical care, lifestyle and diet changes can be controlled. See your rheumatologist and get with a program!





 Everybody wants to maintain optimal height during their adult lifetime. But height loss is a common part of the aging process. We may notice tall elderly people with great posture, but unfortunately, they are a distinct minority.
Everybody wants to maintain optimal height during their adult lifetime. But height loss is a common part of the aging process. We may notice tall elderly people with great posture, but unfortunately, they are a distinct minority.