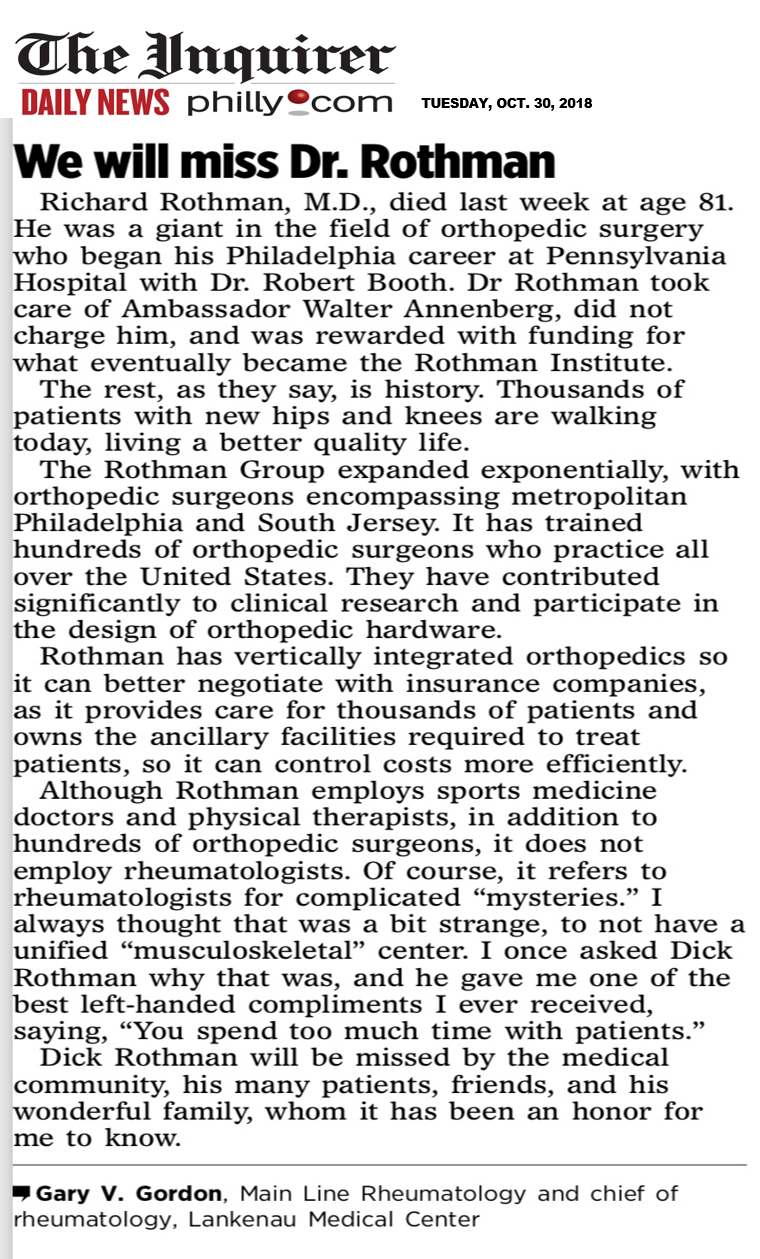
As seen on October 30, 2018 on philly.com and in The Inquirer, a Letter to the Editor written by Dr. Gary Gordon on the death of his medicine colleague, Dr. Richard Rothman.

As seen on October 30, 2018 on philly.com and in The Inquirer, a Letter to the Editor written by Dr. Gary Gordon on the death of his medicine colleague, Dr. Richard Rothman.
To all men over age 50: At your next annual physical checkup visit, ask your doctor to check your height. If you have lost about one inch or more in the past year, you may have male osteoporosis, and is a very noticeable sign.
Osteoporosis is not just a “woman’s disease”. Although osteoporosis is typically  associated with women, it is also diagnosed in men who account for an estimated one in five Americans who have osteoporosis. It is the major cause of fractures in the older population, where bones become thin and brittle, and as a result become weaker and more fragile. Women traditionally experience bone and spine issues after menopause and receive a confirmed diagnosis with a Dexa (bone) scan. However, men are normally not screened for osteoporosis, and don’t learn they have the condition until they experience a fracture. People who have rheumatoid arthritis or who smoke, consume more than three alcoholic drinks a day, have had prolonged prednisone treatment or previously experienced a fracture from only minimal impact should talk to their doctor about starting screening earlier.
associated with women, it is also diagnosed in men who account for an estimated one in five Americans who have osteoporosis. It is the major cause of fractures in the older population, where bones become thin and brittle, and as a result become weaker and more fragile. Women traditionally experience bone and spine issues after menopause and receive a confirmed diagnosis with a Dexa (bone) scan. However, men are normally not screened for osteoporosis, and don’t learn they have the condition until they experience a fracture. People who have rheumatoid arthritis or who smoke, consume more than three alcoholic drinks a day, have had prolonged prednisone treatment or previously experienced a fracture from only minimal impact should talk to their doctor about starting screening earlier.
Be proactive and don’t wait until you experience pain or height loss, before seeking help. Here are some questions to ask yourself.
According to a recent article published by the National Institutes of Health (NIH) Osteoporosis and Related Bone Diseases National Resource Center, here is important osteoporosis information for men.
Risk factors linked to osteoporosis in men:
Osteoporosis can be effectively treated if detected before significant bone loss has occurred. A medical work-up to diagnose osteoporosis includes a complete medical history, x-rays, and urine and blood tests. The doctor may also order a BMD (bone mineral density of DEXA scan) test, which can be used to detect low bone density, predict the risk for future fractures, diagnose osteoporosis and monitor the effectiveness of treatments.
Primary and Secondary Osteoporosis
There are two types of osteoporosis: primary and secondary. Primary osteoporosis is either caused by age-related bone loss (men age 70, and over), or have an unknown cause.
At least half of men with osteoporosis have at least one secondary cause (sometimes more). In cases of secondary osteoporosis, the loss of bone mass is caused by lifestyle behaviors, diseases or medications. The most common causes of secondary osteoporosis in men include exposure to glucocorticoid medication, hypogonadism (low levels of testosterone), alcohol abuse, smoking, gastrointestinal disease, hypercalciuria and immobilization.
Causes of Secondary Osteoporosis in Men
What You Can Do!
Make an appointment with your rheumatologist or endocrinologist for an evaluation and diagnosis. It’s your continued committed partnership in treating your osteoporosis.
Osteoporosis management includes eating foods high in calcium (i.e. dairy products) and taking vitamin D (1,000 mg daily for men age 50-70; 1,200 mg over age 71), regular weight-bearing exercise, no smoking, limitation of alcohol and caffeine consumption, and fall-prevention.
Main Line Rheumatology is more mobile! Our improved mobile website now makes it easier for you to be well informed, every day! Read all about our doctors, get office information, learn more about diseases we treat, read about us in the News, and catch up on daily social media posts ~ all in one place. Come visit!
If you have arthritis, you know about the term “bone on bone”. We tell patients that you cannot grow new cartilage once it is destroyed, whether from over or repetitive use, the  natural aging process, or injury. Stories about stem therapy being used to treat osteoarthritis, an aggressive degenerative form of arthritis, are popular on the internet. But, can stem cells regenerate damaged cartilage with this disease? Maybe one day we can be cautiously optimistic, but for today, I am still skeptical.
natural aging process, or injury. Stories about stem therapy being used to treat osteoarthritis, an aggressive degenerative form of arthritis, are popular on the internet. But, can stem cells regenerate damaged cartilage with this disease? Maybe one day we can be cautiously optimistic, but for today, I am still skeptical.
Our understanding is that stem cells are the building blocks of all human tissue. Arthritis, or joint degeneration, is due to loss of the cartilage that cushions bones and the stem cell goal is to treat arthritis to regrow cartilage.
Stem cells that come from your own body and are harvested through a medical scientific procedure, are then injected back into your body (stem cell therapy) in a desired location, addressing a specific medical condition, movement or pain problem. A newborn baby’s umbilical cord is rich in natural stem cells, and there has been a movement over the last 5-10 years to freeze and save these stem cells for that baby’s (or natural family member) possible health needs.
The human body is a remarkable repair machine. Skin can regenerate, and a small piece of liver transplanted in a human body, grows miraculously to accommodate the body’s needs. But damaged cartilage causing osteoarthritis, does not naturally regenerate. Making degenerated and damaged bones and joints “almost good as new” is more often than not, only the outcome of surgery.
Dr. Shane Shapiro, at the Mayo Clinic Orthopedic Surgery and Center for Regenerative Medicine, published an article in May, 2018 describing how efforts and studies in stem cell regenerative medicine could treat degenerative conditions such as osteoarthritis, changing the course of orthopedic surgery over the coming years. Although research and studies show promise, stem cell treatment for arthritis is not widely available at this time, as is still being researched.
When discussing stem cell therapy, it’s important to understand that pure stem cells are not currently available to U.S. patients outside of a clinical research study. Stem cell therapies currently used outside clinical studies do not contain pure stem cells; they are a mix of a variety of cells with only a very small percentage, stem cells.
A handful of clinical research trials, monitored by the U.S. Food and Drug Administration (FDA), are ongoing at this time to study stem cell treatment for arthritis. The early findings are encouraging for the future. Many stem cell therapies now marketed to patients are conducted without a required FDA biologics license. Also, some forms of stem cell therapies are mislabeled, and do not contain actual living stem cells. These practices cause concern among rheumatologists as these treatments may mislead, or even harm the public.
Research into stem cells and arthritis shows that there are opportunities for stem cell treatment resulting mostly in pain relief and improvement in function, or quality of life. But only a few limited early studies have demonstrated improvement in new cartilage or bone formation needed to cure arthritis, so I am skeptical. Exactly how that cartilage regrowth occurs, or even how pain relief is achieved, is still unknown.
To conclude, here is my opinion. Stem cell therapy, particularly with fetal stem cells, offers great promise for many diseases, including regenerating the damaged cartilage of osteoarthritis. Free standing stem cell clinics that offer treatment, giving you back a few of your mature stem cells for a high cost. As a cautionary tale, The New York Times reported, October 15, 2018, that Harvard University is retracting data that had implied that stem cells had improved cardiac function, when stem cells were placed in the heart. The odds of success currently are minimal, and insurance does not cover this expensive procedure. The “Religious Right” has prevailed upon the last three administrations to toss umbilical cords into the trash instead of utilizing them to save or improve lives. We hope this will change one day, or maybe other countries can lead the way.
Gary V. Gordon, MD, FACP, FACR, Chief of Rheumatology, Lankenau Medical Center, Wynnewood, PA received the 2018 Rheumatologist of the Year Award from The Arthritis Foundation. He is pictured with Holly Maddams, Executive Director of the Arthritis Foundation, Eastern PA. Dr. Gordon was honored on October 5, 2018 at The Arthritis Foundation’s Bone Bash, held at Mutter Museum of The College of Physicians of Philadelphia.
pictured with Holly Maddams, Executive Director of the Arthritis Foundation, Eastern PA. Dr. Gordon was honored on October 5, 2018 at The Arthritis Foundation’s Bone Bash, held at Mutter Museum of The College of Physicians of Philadelphia.